
Respiratory and peripheral muscle involvement in patients with pulmonary arterial hypertension due to congenital heart diseases
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Accepted: 1 December 2020
Authors
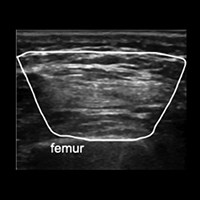
Skeletal and respiratory muscle dysfunction has been previously described in patients with other etiologic subgroups of pulmonary arterial hypertension (PAH) but has never been investigated in patients with PAH due to congenital heart diseases (CHD). This study aims to show the involvement of skeletal and respiratory muscles in these patients. This cross-sectional study included patients with PAH due to CHD and healthy controls. Patients’ demographic properties, six-minute walk tests; shoulder abduction, handgrip, knee extension, and ankle dorsiflexion muscle strength, maximum inspiratory (MIP) and expiratory pressures (MEP) were measured. Deltoid, flexor digitorum superficialis, and profundus, tibialis anterior and rectus femoris muscles were visualized with ultrasonography and their cross-sectional areas (CSA) were also measured in both groups. 12 patients and 12 controls were included. Mean MIP was 104.22±32.57 cm H2O for healthy participants while 61.33±29.74 cm H2O for patients (p<0.001). For mean MEP, it was 100.08±26.05 cm H2O in healthy participants and 69.75±39.79 cmH2O in controls (p=0.004). When the strength of skeletal muscles was compared, there were significant differences between the groups in all measurements except for bilateral grip strength. In the correlation analysis, MIP and MEP values showed no significant correlations with clinical parameters. They showed significant moderate correlations with skeletal muscle strength. When CSAs of the muscles were compared, there were significant differences in all measurements except for left FDS and FDP and bilateral rectus femoris. This study showed that in patients with pulmonary arterial hypertension due to CHD, respiratory muscle strength is significantly worse than healthy participants. Patients had also significantly worse skeletal muscle strength except for grip strength.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.