
The challenging management of a giant intrathoracic desmoid tumour: a case report
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Published: 8 March 2021
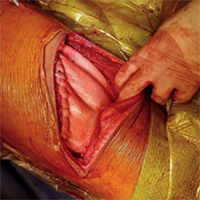
Desmoid tumours are rare, locally aggressive neoplasms exhibiting high tendency for recurrence, even after complete resection. Only 1 in 5 of them originates from the chest wall, usually measuring less than 10 cm at diagnosis. Herein, we report the case of a woman presenting with symptoms of gradual lung compression by a giant desmoid tumour occupying the entire hemithorax. She underwent complete surgical resection of the tumour and chest wall reconstruction. She had disease recurrence 15 months later and currently remains under regular follow-up. The management of intrathoracic desmoid tumours is challenging because they are usually not diagnosed until they become large enough to cause compression symptoms. While medical management is the primary modality of treatment, surgery could be considered in selected cases where significant symptoms arise, and the functional status is impaired secondary to the tumour. Adjuvant radiotherapy to minimise the risk of local recurrence should also be considered.
Downloads
Sakorafas GH, Nissotakis C, Peros G. Abdominal desmoid tumors. Surg Oncol 2007;16:131–42.
McKinnon JG, Neifeld JP, Kay S, et al. Management of desmoid tumors. Surg Gynecol Obstet 1989;169:104–6.
Fletcher CD, Unni KK, Mertens F. Pathology and genetics of tumours of soft tissue and bone. Lyon: IARC Press; 2002.
Shinagare AB, Ramaiya NH, Jagannathan JP, et al. A to Z of desmoid tumors. AJR Am J Roentgenol 2011;197:W1008–14.
Howard JH, Pollock RE. Intra-abdominal and abdominal wall desmoid fibromatosis. Oncol Ther 2016;4:57–72.
Deyrup AT, Tretiakova M, Montag AG. Estrogen receptor-β expression in extraabdominal fibromatoses. Cancer 2006;106:208-13.
Lee JC, Thomas JM, Phillips S, et al. Aggressive fibromatosis: MRI Features with pathologic correlation. AJR Am J Roentgenol 2006;186:247–54.
Koshariya M, Shukla S, Khan Z, et al. Giant desmoid tumor of the anterior abdominal wall in a young female: a case report. Case Rep Surg 2013;2013:780862.
Kovačević K, Obad-Kovačević D, Popić-Ramač J. Sporadic giant intra-abdominal desmoid tumor: A radiological case report. Mol. Clin. Oncol. 2017;6:896–8.
Weiss SW, Goldblum JR. Fibromatoses. In: Weiss SW, Goldblum JR, editors. Enzinger and Weiss’s soft tissue tumors. St. Louis: Mosby; 2001. p. 309–46.
Kasper B, Baumgarten C, Bonvalot S, et al. Management of sporadic desmoid-type fibromatosis: A European consensus approach based on patients’ and professionals’ expertise – A Sarcoma Patients EuroNet and European Organisation for Research and Treatment of Cancer/Soft Tissue and Bone Sarcoma Group. Eur J Cancer 2015;51:127–36.
Kasper B, Baumgarten C, Garcia J, et al. An update on the management of sporadic desmoid-type fibromatosis: a European Consensus Initiative between Sarcoma PAtients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Ann Oncol 2017;28:2399–408.
Briand S, Barbier O, Biau D, et al. Wait-and- see policy as a first-line management for extra-abdominal desmoid tumors. J Bone Joint Surg Am 2014;96:631–8.
Fiore M, Rimareix F, Mariani L, et al. Desmoid-type fibromatosis: A front-line conservative approach to select patients for surgical treatment. Ann Surg Oncol 2009;16:2587–93.
Bonvalot S, Eldweny H, Haddad V, et al. Extra-abdominal primary fibromatosis: Aggressive management could be avoided in a subgroup of patients. Eur J Surg Oncol 2008;34:462–8.
Colombo C, Miceli R, Le Péchoux C, et al. Sporadic extra abdominal wall desmoid-type fibromatosis: Surgical resection can be safely limited to a minority of patients. Eur J Cancer 2015;51:186–92.
Bonvalot S, Ternès N, Fiore M, et al. Spontaneous regression of primary abdominal wall desmoid tumors: More common than previously thought. Ann Surg Oncol 2013;20:4096–102.
Roussin S, Mazouni C, Rimareix F, et al. Toward a new strategy in desmoid of the breast? Eur J Surg Oncol 2015;41:571–6.
Joglekar SB, Rose PS, Sim F, et al. Current perspectives on desmoid tumors: the mayo clinic approach. Cancers (Basel) 2011;3:3143–55.
Micke O, Seegenschmiedt MH, German Cooperative Group on Radiotherapy for Benign Diseases. Radiation therapy for aggressive fibromatosis (desmoid tumors): Results of a national patterns of Care Study. Int J Radiat Oncol 2005;61:882–91.
How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.