
Takotsubo syndrome and pheochromocytoma: an insidious combination
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
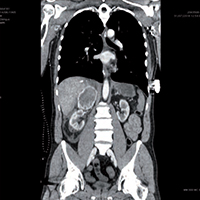
Pheochromocytoma is a rare adrenal tumor characterized by the secretion of catecholamines and vasoactive peptides. It can cause a catecholaminergic storm and lead to acute coronary syndromes. We present the case of a 53-year-old man, without any medical history, who arrived to the hospital following a spinal trauma due a fall. He presents back and retrosternal pain, with a clinical status of acute pulmonary edema, sinus tachycardia with left bundle branch block, left ventricular apical ballooning with depressed systolic function. Blood tests show a very important increase of Troponin and transaminases. A contrast chest-abdomen CT highlighted a right adrenal solid mass, with a diameter of 78mm, partial capsular laceration, compression of the inferior vena cava and the hepatic parenchyma. The clinical condition of the patient rapidly worsens from a respiratory and hemodynamic point of view, with cardiogenic shock, anuria and sepsis, refractory to all the medical treatments, until the patient died. The autopsy confirmed that the abdominal mass was a pheochromocytoma, broken after the trauma suffered. The resulting catecholaminergic storm caused a myocardial ischemia with Takotsubo syndrome, with cardiogenic shock. This unfortunate case confirms the pheochromocytoma as important risk factor for the onset of Takotsubo syndrome, and the how dramatic and severe a catecholaminergic storm can be.
Altmetrics
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.