Right-sided infective endocarditis and pulmonary embolism: a multicenter study
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
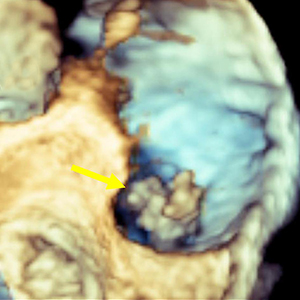
The incidence of right-sided infective endocarditis (RSIE) is steadily increasing and it has been reported to be associated with high risk of embolic events (EE). Aim of our study was to identify the clinical characteristics of patients with RSIE complicated by PE. Indeed, the identification of patients at high risk of significant PE who will benefit from a more aggressive therapeutic strategy may improve the prognosis. From January 2015 to September 2020, 176 patients (Pts) in 6 centers were found to have definite RSIE complicated by PE. Advanced imaging for PE including computed tomography pulmonary angiography (CTPA) was performed in 28 pts (16%) who represent our study group (24 male, mean age 50.6 ±18.29 years). They all underwent transesophageal echocardiography (TEE), in 12 cases (43%) also three-dimensional (3D) TEE, and 27 patients (99%) had both TEE and transthoracic echocardiography (TTE). A total of 53 vegetations (V) were detected. In 18 pts (64%) two or more vegetations were found. Native tricuspid valve was the most frequently involved valve (38 V, 71.7%), followed by catheter (5 V, 9.4%), tricuspid valve prosthesis (4 V, 7.5%), chordae and papillary muscle (2 V, 3.8%) and one vegetation (9%) in each of the following: pulmonic valve, inferior vena cava, eustachian valve, and right atrium. The most common location for vegetations was the anterior leaflet of the tricuspid valve (19 V, 35.8 %) followed by the posterior leaflet (11 V, 20.8%). The most common vegetations morphology was raceme-like shaped (35.8%). Staphylococcus aureus (S. aureus) was the most common causative pathogen (14 pts, 50%). The incidence of PE was very high in patients with vegetation length above 1.5 cm (median 17.6±6.5 mm by TEE). Our results suggest that a routine CTPA should be advised in the presence of vegetations larger than 1.5 cm and with S. aureus infection. This behavior would identify patients at high risk of PE who will benefit from a more aggressive therapeutic strategy, leading to an improvement in the prognosis. Further prospective studies are required to better confirm our hypothesis.




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- Paolo Ruggeri, Federica Lo Bello, Francesco Nucera, Michele Gaeta, Francesco Monaco, Gaetano Caramori, Giuseppe Girbino, Hereditary hyperhomocysteinemia associated with nephrotic syndrome complicated by artery thrombosis and chronic thromboembolic pulmonary hypertension: A case report , Monaldi Archives for Chest Disease: Vol. 87 No. 3 (2017)
- Massimiliano Polastri, Lara Pisani, Andrea Dell'Amore, Stefano Nava, Revolving door respiratory patients: A rehabilitative perspective , Monaldi Archives for Chest Disease: Vol. 87 No. 3 (2017)
- Z. Celebi Sözener, A. Kaya, C. Atasoy, M. Kılıckap, N. Numanoglu, I. Savas, Septic Pulmonary Embolism: three Case Reports , Monaldi Archives for Chest Disease: Vol. 69 No. 2 (2008): Pulmonary series
- Abhishekl Agarwal, Sakshi Batra, Rajendra Prasad, Anand Verma, Abdul Q. Jilani, Surya Kant, A study on the prevalence of depression and the severity of depression in patients of chronic obstructive pulmonary disease in a semi-urban Indian population , Monaldi Archives for Chest Disease: Vol. 88 No. 1 (2018)
- Abhijeet Singh, Rajendra Prasad, Rajiv Garg, Surya Kant, Giridhar B. Hosmane, Abhisek Dubey, Abhisek Agarwal, Ram Kishun Verma, A study to estimate prevalence and risk factors of Obstructive Sleep Apnoea Syndrome in a semi-urban Indian population , Monaldi Archives for Chest Disease: Vol. 87 No. 1 (2017)
- Dimitrios Papadopoulos, Panagiotis Misthos, Maria Chorti, Vlasios Skopas, Alexandra Nakou, Napoleon Karagianidis, Achilleas Lioulias, Vasiliki Filaditaki, Unilateral pulmonary hypoplasia in an adult patient , Monaldi Archives for Chest Disease: Vol. 88 No. 1 (2018)
- Madalina Macrea, Richard ZuWallack, Linda Nici, There’s no place like home: Integrating pulmonary rehabilitation into the home setting , Monaldi Archives for Chest Disease: Vol. 87 No. 2 (2017)
- Oscar Serafini, Francesco Greco, Gianfranco Misuraca, Mario Chiatto, Antonino Buffon, Echocardiography in the diagnostic and prognostic evaluation of thromboembolic pulmonary hypertension , Monaldi Archives for Chest Disease: Vol. 64 No. 2 (2005): Cardiac series
- Vishal Chopra, Hardik Jain, Akhil D. Goel, Siddharth Chopra, Ashrafjit S. Chahal, Neha Garg, Vidhu Mittal, Correlation of aspergillus skin hypersensitivity with the duration and severity of asthma , Monaldi Archives for Chest Disease: Vol. 87 No. 3 (2017)
- Cuneyt Tetikkurt, Nail Yılmaz, Seza Tetikkurt, Şule Gundogdu, Rian Disci, The value of exfoliative cell cytology in the diagnosis of exudative pleural effusions , Monaldi Archives for Chest Disease: Vol. 88 No. 3 (2018)
You may also start an advanced similarity search for this article.
