Respiratory and peripheral muscle involvement in patients with pulmonary arterial hypertension due to congenital heart diseases
Accepted: December 1, 2020
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
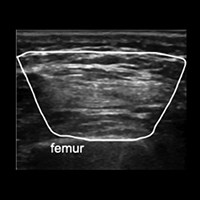
Skeletal and respiratory muscle dysfunction has been previously described in patients with other etiologic subgroups of pulmonary arterial hypertension (PAH) but has never been investigated in patients with PAH due to congenital heart diseases (CHD). This study aims to show the involvement of skeletal and respiratory muscles in these patients. This cross-sectional study included patients with PAH due to CHD and healthy controls. Patients’ demographic properties, six-minute walk tests; shoulder abduction, handgrip, knee extension, and ankle dorsiflexion muscle strength, maximum inspiratory (MIP) and expiratory pressures (MEP) were measured. Deltoid, flexor digitorum superficialis, and profundus, tibialis anterior and rectus femoris muscles were visualized with ultrasonography and their cross-sectional areas (CSA) were also measured in both groups. 12 patients and 12 controls were included. Mean MIP was 104.22±32.57 cm H2O for healthy participants while 61.33±29.74 cm H2O for patients (p<0.001). For mean MEP, it was 100.08±26.05 cm H2O in healthy participants and 69.75±39.79 cmH2O in controls (p=0.004). When the strength of skeletal muscles was compared, there were significant differences between the groups in all measurements except for bilateral grip strength. In the correlation analysis, MIP and MEP values showed no significant correlations with clinical parameters. They showed significant moderate correlations with skeletal muscle strength. When CSAs of the muscles were compared, there were significant differences in all measurements except for left FDS and FDP and bilateral rectus femoris. This study showed that in patients with pulmonary arterial hypertension due to CHD, respiratory muscle strength is significantly worse than healthy participants. Patients had also significantly worse skeletal muscle strength except for grip strength.




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- Paolo Ruggeri, Federica Lo Bello, Francesco Nucera, Michele Gaeta, Francesco Monaco, Gaetano Caramori, Giuseppe Girbino, Hereditary hyperhomocysteinemia associated with nephrotic syndrome complicated by artery thrombosis and chronic thromboembolic pulmonary hypertension: A case report , Monaldi Archives for Chest Disease: Vol. 87 No. 3 (2017)
- Massimiliano Polastri, Lara Pisani, Andrea Dell'Amore, Stefano Nava, Revolving door respiratory patients: A rehabilitative perspective , Monaldi Archives for Chest Disease: Vol. 87 No. 3 (2017)
- Berardo Sarubbi, Giancarlo Scognamiglio, Flavia Fusco, Enrico Melillo, Michele D'Alto, Maria Giovanna Russo, A “long-standing†malpositioned pacing lead. Long-term follow-up after extraction , Monaldi Archives for Chest Disease: Vol. 88 No. 3 (2018)
- Halil Yanardag, Cuneyt Tetikkurt, Muammer Bilir, Clinical and prognostic significance of muscle biopsy in sarcoidosis , Monaldi Archives for Chest Disease: Vol. 88 No. 1 (2018)
- Abhishekl Agarwal, Sakshi Batra, Rajendra Prasad, Anand Verma, Abdul Q. Jilani, Surya Kant, A study on the prevalence of depression and the severity of depression in patients of chronic obstructive pulmonary disease in a semi-urban Indian population , Monaldi Archives for Chest Disease: Vol. 88 No. 1 (2018)
- Alfonso Sforza, Maria V. Carlino, Giovanni Albano, Maria I. Arnone, Giuliano De Stefano, Andrea D'Amato, Federica De Pisapia, Giovanni de Simone, Costantino Mancusi, A challenging diagnosis of dyspnea: A case report of contralateral reexpansion pulmonary edema , Monaldi Archives for Chest Disease: Vol. 88 No. 1 (2018)
- Abhijeet Singh, Rajendra Prasad, Rajiv Garg, Surya Kant, Giridhar B. Hosmane, Abhisek Dubey, Abhisek Agarwal, Ram Kishun Verma, A study to estimate prevalence and risk factors of Obstructive Sleep Apnoea Syndrome in a semi-urban Indian population , Monaldi Archives for Chest Disease: Vol. 87 No. 1 (2017)
- Michele Correale, Deodata Montrone, Donato Lacedonia, Riccardo Ieva, Romano Bucci, Addolorata Corrado, Francesco Paolo Cantatore, Carmen Adriana Greco, Morena Concilio, Gaetano Serviddio, Maria Pia Foschino Barbaro, Matteo Di Biase, Natale Daniele Brunetti, Multiprofessional and Intrahospital Experience for Diagnosis and Treatment of Pulmonary Arterial Hypertension , Monaldi Archives for Chest Disease: Vol. 78 No. 4 (2012): Cardiac series
- Sergio C. Conte, Giulia Spagnol, Marco Confalonieri, Beatrice Brizi, Deep sedation versus minimal sedation during endobronchial ultrasound transbronchial needle aspiration , Monaldi Archives for Chest Disease: Vol. 88 No. 3 (2018)
- Alberto Genovesi Ebert, Furio Colivicchi, Marco Malvezzi Caracciolo, Carmine Riccio, Additive beneficial effects of beta blockers in the prevention of symptomatic heart failure , Monaldi Archives for Chest Disease: Vol. 72 No. 1 (2009): Cardiac series
You may also start an advanced similarity search for this article.
