Respiratory and peripheral muscle involvement in patients with pulmonary arterial hypertension due to congenital heart diseases
Accepted: December 1, 2020
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
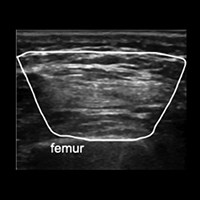
Skeletal and respiratory muscle dysfunction has been previously described in patients with other etiologic subgroups of pulmonary arterial hypertension (PAH) but has never been investigated in patients with PAH due to congenital heart diseases (CHD). This study aims to show the involvement of skeletal and respiratory muscles in these patients. This cross-sectional study included patients with PAH due to CHD and healthy controls. Patients’ demographic properties, six-minute walk tests; shoulder abduction, handgrip, knee extension, and ankle dorsiflexion muscle strength, maximum inspiratory (MIP) and expiratory pressures (MEP) were measured. Deltoid, flexor digitorum superficialis, and profundus, tibialis anterior and rectus femoris muscles were visualized with ultrasonography and their cross-sectional areas (CSA) were also measured in both groups. 12 patients and 12 controls were included. Mean MIP was 104.22±32.57 cm H2O for healthy participants while 61.33±29.74 cm H2O for patients (p<0.001). For mean MEP, it was 100.08±26.05 cm H2O in healthy participants and 69.75±39.79 cmH2O in controls (p=0.004). When the strength of skeletal muscles was compared, there were significant differences between the groups in all measurements except for bilateral grip strength. In the correlation analysis, MIP and MEP values showed no significant correlations with clinical parameters. They showed significant moderate correlations with skeletal muscle strength. When CSAs of the muscles were compared, there were significant differences in all measurements except for left FDS and FDP and bilateral rectus femoris. This study showed that in patients with pulmonary arterial hypertension due to CHD, respiratory muscle strength is significantly worse than healthy participants. Patients had also significantly worse skeletal muscle strength except for grip strength.




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- Shekhar Kunal, Vijay Pathak, Keshav Pathak, Monika Mishra, Shashi Mohan Sharma, Sudhir Bhandari, Very late stent thrombosis associated with COVID-19 infection: a case report and review of the literature , Monaldi Archives for Chest Disease: Vol. 92 No. 2 (2022)
- Christopher Ull, Mirko Aach, Josef Reichert, Thomas Armin Schildhauer, Justyna Swol, Successful non-surgical management of pleuroparenchymal fistula following cervical intraspinal empyema , Monaldi Archives for Chest Disease: Vol. 88 No. 1 (2018)
- Irappa Madabhavi, Malay Sarkar, Nagaveni Kadakol, COVID-19: a review , Monaldi Archives for Chest Disease: Vol. 90 No. 2 (2020)
- Diana Alexandra Gonçalves Pimenta, Renata Carvalho, Raquel Pereira, Rui Rolo, Lurdes Ferreira, Interstitial nephritis secondary to treatment with pembrolizumab, a rare complication in two patients with lung adenocarcinoma , Monaldi Archives for Chest Disease: Vol. 93 No. 2 (2023)
- Debapriya Maji, Upasna Agarwal, Lokender Kumar, Vinay V, Amit Sharma, Clinicodemographic profile and outcome of tuberculosis treatment in TB-HIV co-infected patients receiving daily ATT under a single window TB-HIV services delivery initiative , Monaldi Archives for Chest Disease: Vol. 93 No. 3 (2023)
- Garyfallia Pepera, Εfstratios Xanthos, Andreas Lilios, Theodoros Xanthos, Knowledge of cardiopulmonary resuscitation among Greek physiotherapists , Monaldi Archives for Chest Disease: Vol. 89 No. 3 (2019)
- Massimiliano Polastri, Giulia Zagnoni, Antonio Loforte, Basic movements for postoperative exercise in patients with left ventricular assist devices , Monaldi Archives for Chest Disease: Vol. 89 No. 1 (2019)
- Carlo Vigorito, Pompilio Faggiano, Gian Francesco Mureddu, COVID-19 pandemic: what consequences for cardiac rehabilitation? , Monaldi Archives for Chest Disease: Vol. 90 No. 1 (2020)
- The Publisher, Correction. Robotic resection of mediastinal left vagus neurofibroma , Monaldi Archives for Chest Disease: Vol. 93 No. 1 (2023)
- Mario Tamburrini, Parikshit Thakare, Francesca Zampieri, Angelo Scarda, Alessandra Di Paolo, Giancarlo De Leo, Enrico Gianfagna, Lucia Vietri, Umberto Zuccon, A case report on expanding horizon of endobronchial ultrasound through esophagus , Monaldi Archives for Chest Disease: Vol. 90 No. 3 (2020)
<< < 92 93 94 95 96 97 98 99 100 101 > >>
You may also start an advanced similarity search for this article.
