The challenging management of a giant intrathoracic desmoid tumour: a case report
Accepted: February 24, 2021
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
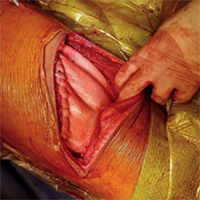
Desmoid tumours are rare, locally aggressive neoplasms exhibiting high tendency for recurrence, even after complete resection. Only 1 in 5 of them originates from the chest wall, usually measuring less than 10 cm at diagnosis. Herein, we report the case of a woman presenting with symptoms of gradual lung compression by a giant desmoid tumour occupying the entire hemithorax. She underwent complete surgical resection of the tumour and chest wall reconstruction. She had disease recurrence 15 months later and currently remains under regular follow-up. The management of intrathoracic desmoid tumours is challenging because they are usually not diagnosed until they become large enough to cause compression symptoms. While medical management is the primary modality of treatment, surgery could be considered in selected cases where significant symptoms arise, and the functional status is impaired secondary to the tumour. Adjuvant radiotherapy to minimise the risk of local recurrence should also be considered.




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- Elena Sogaro, Francesca Schininà , Costanza Burgisser, Francesco Orso, Rachele Pallante, Teresa Aloi, Duccio Vanni, Adolfo Pazzagli, Francesco Fattirolli, Type D personality impairs Quality of Life, coping and short-term psychological outcome in patients attending an outpatient intensive program of cardiac rehabilitation , Monaldi Archives for Chest Disease: Vol. 74 No. 4 (2010): Cardiac series
- Paolo Ruggeri, Federica Lo Bello, Francesco Nucera, Michele Gaeta, Francesco Monaco, Gaetano Caramori, Giuseppe Girbino, Hereditary hyperhomocysteinemia associated with nephrotic syndrome complicated by artery thrombosis and chronic thromboembolic pulmonary hypertension: A case report , Monaldi Archives for Chest Disease: Vol. 87 No. 3 (2017)
- Z. Celebi Sözener, A. Kaya, C. Atasoy, M. Kılıckap, N. Numanoglu, I. Savas, Septic Pulmonary Embolism: three Case Reports , Monaldi Archives for Chest Disease: Vol. 69 No. 2 (2008): Pulmonary series
- William Newmarch, Angelica Puopolo, Madina Weiler, Brian Casserly, Hamman-Rich syndrome: a forgotten entity , Monaldi Archives for Chest Disease: Vol. 87 No. 1 (2017)
- C. Zisis, S. Fragoulis, D. Rontogianni, G. Stratakos, I. Bellenis, Malignant triton tumour of the anterior mediastinum as incidental finding , Monaldi Archives for Chest Disease: Vol. 65 No. 4 (2006): Pulmonary series
- Davide Zampieri, Alessandro Pangoni, Giuseppe Marulli, Federico Rea, Acquired tracheoesophageal fistula repair, due to prolonged mechanical ventilation, in patient with double incomplete aortic arch , Monaldi Archives for Chest Disease: Vol. 88 No. 3 (2018)
- Yeliz Akturk, Serra Ozbal Günes, Baki Hekimoglu, A rib abnormality mimicking pulmonary nodule: a pitfall in the plain chest x-ray , Monaldi Archives for Chest Disease: Vol. 81 No. 1-2 (2015): Pulmonary series
- F. Iaselli, G. Rea, S. Cappabianca, G. Fabozzi, M. Montemarano, C. Vitale, A.A. Stanziola, R. Muto, A. Rotondo, Adult-onset pulmonary involvement in Niemann-Pick disease type B , Monaldi Archives for Chest Disease: Vol. 75 No. 4 (2011): Pulmonary series
- P.A. Canessa, L. Pratticò, M. Sivori, P. Magistrelli, F. Fedeli, A. Cavazza, G. Calcina, Acute Fibrinous and Organising Pneumonia in Whipple’s disease , Monaldi Archives for Chest Disease: Vol. 69 No. 4 (2008): Pulmonary series
- K. Psathakis, V. Skouras, F. Chatzivassiloglou, K. Tsintiris, Osteophytes may be a rare cause of recurrent pleural effusions , Monaldi Archives for Chest Disease: Vol. 79 No. 2 (2013): Pulmonary series
You may also start an advanced similarity search for this article.
