The challenging management of a giant intrathoracic desmoid tumour: a case report
Accepted: February 24, 2021
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
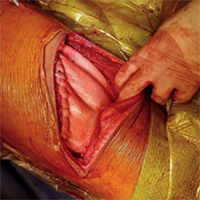
Desmoid tumours are rare, locally aggressive neoplasms exhibiting high tendency for recurrence, even after complete resection. Only 1 in 5 of them originates from the chest wall, usually measuring less than 10 cm at diagnosis. Herein, we report the case of a woman presenting with symptoms of gradual lung compression by a giant desmoid tumour occupying the entire hemithorax. She underwent complete surgical resection of the tumour and chest wall reconstruction. She had disease recurrence 15 months later and currently remains under regular follow-up. The management of intrathoracic desmoid tumours is challenging because they are usually not diagnosed until they become large enough to cause compression symptoms. While medical management is the primary modality of treatment, surgery could be considered in selected cases where significant symptoms arise, and the functional status is impaired secondary to the tumour. Adjuvant radiotherapy to minimise the risk of local recurrence should also be considered.




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- I.A. Brownlee, A. Aseeri, C. Ward, J.P. Pearson, From gastric aspiration to airway inflammation , Monaldi Archives for Chest Disease: Vol. 73 No. 2 (2010): Pulmonary series
- S. Conforti, M. Torre, S. Fieschi, A. Lomonaco, M. Ravini, Successful treatment of persistent postoperative air leaks following the placement of an endobronchial one-way valve , Monaldi Archives for Chest Disease: Vol. 73 No. 2 (2010): Pulmonary series
- S. Aliberti, M.C. Andrisani, P. Tarsia, R. Trevisan, R. Cosentini, L. Longhi, M. Pappalettera, M. Nosotti, F. Blasi, Non-invasive continuous positive airway pressure in monolateral lung transplant patient with pneumonia and IPF , Monaldi Archives for Chest Disease: Vol. 73 No. 4 (2010): Pulmonary series
- R. Trisolini, After all, everybody loves a good story! Update on the Case Reports’ Chronicle , Monaldi Archives for Chest Disease: Vol. 75 No. 4 (2011): Pulmonary series
- A.J. Lopes, T.T. Mafort, A. de Sá Ferreira, M.C. Santos de Castro, M. de Cássia Firmida, E. de Andrade Marques, Is the type of chronic pulmonary infection a determinant of lung function outcomes in adult patients with cystic fibrosis? , Monaldi Archives for Chest Disease: Vol. 77 No. 3-4 (2012): Pulmonary series
- Vito Maurizio Parato, Germana Gizzi, Simone D'Agostino, Simona Pelliccioni, Michele Scarano, An unusual case of severe left ventricle outflow tract obstruction due to a coexistence of Takotsubo cardiomyopathy with septal hypertrophic cardiomyopathy , Monaldi Archives for Chest Disease: Vol. 92 No. 3 (2022)
- M. Confalonieri, M. Kodric, M. Santagiuliana, C. Longo, M. Biolo, R. Cifaldi, C. Torregiani, M. Jevnikar, To use or not to use corticosteroids for pneumonia? A clinician’s perspective , Monaldi Archives for Chest Disease: Vol. 77 No. 2 (2012): Pulmonary series
- Christophoros Kotoulas, Vasileios Tzilalis, Emmanouil Spyridakis, Ioannis Mamarelis, Endovascular management of a late saccular aortic aneurysm after end-to-end repair of coarctation , Monaldi Archives for Chest Disease: Vol. 76 No. 4 (2011): Cardiac series
- Luca Degli Esposti, Diego Sangiorgi, Marcello Arca, Giovanni B. Vigna, Stefano Buda, Ezio Degli Esposti, Achievement of therapeutic target in subjects on statin treatment in clinical practice. Results of the STAR (Statins Target Assessment in Real practice) study , Monaldi Archives for Chest Disease: Vol. 76 No. 4 (2011): Cardiac series
- C. Carbonelli, S. Montepietra, A. Caruso, A. Cavazza, C. Feo, F. Menzella, L. Motti, L. Zucchi, Sarcoidosis and multiple sclerosis: systemic toxicity associated with the use of interferon-beta therapy , Monaldi Archives for Chest Disease: Vol. 77 No. 1 (2012): Pulmonary series
<< < 25 26 27 28 29 30 31 32 33 34 > >>
You may also start an advanced similarity search for this article.
