Takotsubo syndrome and pheochromocytoma: an insidious combination
Accepted: March 2, 2021
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
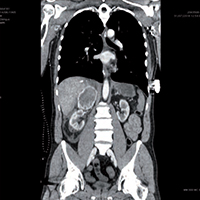
Pheochromocytoma is a rare adrenal tumor characterized by the secretion of catecholamines and vasoactive peptides. It can cause a catecholaminergic storm and lead to acute coronary syndromes. We present the case of a 53-year-old man, without any medical history, who arrived to the hospital following a spinal trauma due a fall. He presents back and retrosternal pain, with a clinical status of acute pulmonary edema, sinus tachycardia with left bundle branch block, left ventricular apical ballooning with depressed systolic function. Blood tests show a very important increase of Troponin and transaminases. A contrast chest-abdomen CT highlighted a right adrenal solid mass, with a diameter of 78mm, partial capsular laceration, compression of the inferior vena cava and the hepatic parenchyma. The clinical condition of the patient rapidly worsens from a respiratory and hemodynamic point of view, with cardiogenic shock, anuria and sepsis, refractory to all the medical treatments, until the patient died. The autopsy confirmed that the abdominal mass was a pheochromocytoma, broken after the trauma suffered. The resulting catecholaminergic storm caused a myocardial ischemia with Takotsubo syndrome, with cardiogenic shock. This unfortunate case confirms the pheochromocytoma as important risk factor for the onset of Takotsubo syndrome, and the how dramatic and severe a catecholaminergic storm can be.




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- Gabriele Valli, Francesca De Marco, Maria Teresa Spina, Valentina Valeriano, Antonello Rosa, Valentina Minerva, Enrico Mirante, Maria Pia Ruggieri, Francesco Rocco Pugliese, A pilot study on the application of the current European guidelines for the management of acute coronary syndrome without elevation of ST segment (NSTEMI) in the Emergency Department setting in the Italian region Lazio , Monaldi Archives for Chest Disease: Vol. 82 No. 4 (2014): Cardiac series
- Panagiotis Hountis, Maria Chounti, Chilaiditi’s sign or syndrome? Diagnostic question in two patients with concurrent cardiovascular diseases , Monaldi Archives for Chest Disease: Vol. 87 No. 2 (2017)
- Paola Gremigni, Cynical hostility and the metabolic syndrome: A case-control study , Monaldi Archives for Chest Disease: Vol. 66 No. 3 (2006): Cardiac series
- Massimiliano Polastri, Lara Pisani, Andrea Dell'Amore, Stefano Nava, Revolving door respiratory patients: A rehabilitative perspective , Monaldi Archives for Chest Disease: Vol. 87 No. 3 (2017)
- Muhammad Ijaz, Muhammad Jaffar Khan, Jawad Khan, . Usama, Association of clinical characteristics of patients presenting with influenza like illness or severe acute respiratory illness with development of acute respiratory distress syndrome , Monaldi Archives for Chest Disease: Vol. 87 No. 1 (2017)
- Paolo Ruggeri, Federica Lo Bello, Francesco Nucera, Michele Gaeta, Francesco Monaco, Gaetano Caramori, Giuseppe Girbino, Hereditary hyperhomocysteinemia associated with nephrotic syndrome complicated by artery thrombosis and chronic thromboembolic pulmonary hypertension: A case report , Monaldi Archives for Chest Disease: Vol. 87 No. 3 (2017)
- Edoardo Sciatti, Enrico Vizzardi, Dario S. Cani, Assunta Castiello, Ivano Bonadei, Daria Savoldi, Marco Metra, Antonio D'Aloia, Kounis syndrome, a disease to know: Case report and review of the literature , Monaldi Archives for Chest Disease: Vol. 88 No. 1 (2018)
- Roberto Porta, Laura Comini, Luca Barbano, Luca Bianchi, Michele Vitacca, A case of obstructive sleep apnea syndrome associated with floppy eyelid syndrome: positive effect of CPAP therapy , Monaldi Archives for Chest Disease: Vol. 87 No. 1 (2017)
- Angelo Compare, Riccardo Proietti, Domenico Del Forno, Alessandra Vitelli, Alessandra Grieco, Luigi Maresca, Francesco Giallauria, Vulnerable personality and Takotsubo cardiomyopathy consequent to emotional stressful events: a clinical case report , Monaldi Archives for Chest Disease: Vol. 76 No. 2 (2011): Cardiac series
- Kevin John, Amos Lal, Ajay Mishra, A review of the presentation and outcome of Takotsubo cardiomyopathy in COVID-19 , Monaldi Archives for Chest Disease: Vol. 91 No. 3 (2021)
You may also start an advanced similarity search for this article.
