Takotsubo syndrome and pheochromocytoma: an insidious combination
Accepted: March 2, 2021
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
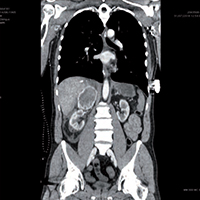
Pheochromocytoma is a rare adrenal tumor characterized by the secretion of catecholamines and vasoactive peptides. It can cause a catecholaminergic storm and lead to acute coronary syndromes. We present the case of a 53-year-old man, without any medical history, who arrived to the hospital following a spinal trauma due a fall. He presents back and retrosternal pain, with a clinical status of acute pulmonary edema, sinus tachycardia with left bundle branch block, left ventricular apical ballooning with depressed systolic function. Blood tests show a very important increase of Troponin and transaminases. A contrast chest-abdomen CT highlighted a right adrenal solid mass, with a diameter of 78mm, partial capsular laceration, compression of the inferior vena cava and the hepatic parenchyma. The clinical condition of the patient rapidly worsens from a respiratory and hemodynamic point of view, with cardiogenic shock, anuria and sepsis, refractory to all the medical treatments, until the patient died. The autopsy confirmed that the abdominal mass was a pheochromocytoma, broken after the trauma suffered. The resulting catecholaminergic storm caused a myocardial ischemia with Takotsubo syndrome, with cardiogenic shock. This unfortunate case confirms the pheochromocytoma as important risk factor for the onset of Takotsubo syndrome, and the how dramatic and severe a catecholaminergic storm can be.




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- Andrea Segreti, Francesco Piccirillo, Simone Pasquale Crispino, Francesca Cocchia, Arianna Martucciello, Vito Calabrese, Fiorella Gurrieri, Francesco Grigioni, Simultaneous presence of Brugada and overgrowth syndromes , Monaldi Archives for Chest Disease: Vol. 94 No. 1 (2024)
- Rita Costa, Antonio Esquinas , Predictors of post-COVID syndrome. Getting ready for the future , Monaldi Archives for Chest Disease: Vol. 93 No. 3 (2023)
- Francesco Natale, Riccardo Molinari, Simona Covino, Roberta Alfieri, Giovanni Cimmino, The cardiac paradox of losing weight: a case of gastro-cardiac syndrome , Monaldi Archives for Chest Disease: Vol. 93 No. 2 (2023)
- Francesco Fattirolli, Alessandra Pratesi, Cardiovascular prevention and rehabilitation in the elderly: evidence for cardiac rehabilitation after myocardial infarction or chronic heart failure , Monaldi Archives for Chest Disease: Vol. 84 No. 1-2 (2015): Cardiac series
- William Newmarch, Angelica Puopolo, Madina Weiler, Brian Casserly, Hamman-Rich syndrome: a forgotten entity , Monaldi Archives for Chest Disease: Vol. 87 No. 1 (2017)
- Shweta Anand, Anshul Jain, Dipti Gothi, Sameer Vaidya, Rambabu Sah, Prevalence, risk factors and effects of restless legs syndrome in COPD patients , Monaldi Archives for Chest Disease: Vol. 93 No. 1 (2023)
- Hazuki Fujimoto, Yohei Kanzawa, Hidemine Senba, Tetsuo Washio, Yukiko Kato, Kei Kawano, Shimpei Mizuki, Jun Ohnishi, Takahiro Nakajima, Naoto Ishimaru, Saori Kinami, Hemophagocytic syndrome in a patient with long-term stable pulmonary sarcoidosis with progressive spleen and bone marrow lesion , Monaldi Archives for Chest Disease: Vol. 93 No. 4 (2023)
- Mamta Singh, Kunal Deokar, Bibhuti Prassan Sinha, Monika Keena, Govind Desai, Ocular manifestations of common pulmonary diseases: a narrative review , Monaldi Archives for Chest Disease: Vol. 94 No. 1 (2024)
- Laura Casaretti, Stefania Paolillo, Roberto Formisano, Ada Bologna, Giacomo Mattiello, Sirio Conte, Laura Petraglia, Francesco Lo Iudice, Irma Fabiani, Anna Paola Cirillo, Alice Vitagliano, Francesco Gambardella, Giuseppe Luca della Ratta, Pasquale Perrone Filardi, Metabolic and cardiovascular effects of combined antiretroviral therapy in patients with HIV infection. Systematic review of literature , Monaldi Archives for Chest Disease: Vol. 76 No. 4 (2011): Cardiac series
- Anu Anna George, Kevin John John, Anil Jha, Ajay Kumar Mishra, Infections precipitating Takotsubo cardiomyopathy, an uncommon complication of a common infection , Monaldi Archives for Chest Disease: Vol. 93 No. 3 (2023)
<< < 3 4 5 6 7 8 9 10 11 12 > >>
You may also start an advanced similarity search for this article.
