Right-sided infective endocarditis and pulmonary embolism: a multicenter study
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
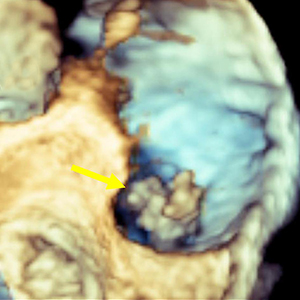
The incidence of right-sided infective endocarditis (RSIE) is steadily increasing and it has been reported to be associated with high risk of embolic events (EE). Aim of our study was to identify the clinical characteristics of patients with RSIE complicated by PE. Indeed, the identification of patients at high risk of significant PE who will benefit from a more aggressive therapeutic strategy may improve the prognosis. From January 2015 to September 2020, 176 patients (Pts) in 6 centers were found to have definite RSIE complicated by PE. Advanced imaging for PE including computed tomography pulmonary angiography (CTPA) was performed in 28 pts (16%) who represent our study group (24 male, mean age 50.6 ±18.29 years). They all underwent transesophageal echocardiography (TEE), in 12 cases (43%) also three-dimensional (3D) TEE, and 27 patients (99%) had both TEE and transthoracic echocardiography (TTE). A total of 53 vegetations (V) were detected. In 18 pts (64%) two or more vegetations were found. Native tricuspid valve was the most frequently involved valve (38 V, 71.7%), followed by catheter (5 V, 9.4%), tricuspid valve prosthesis (4 V, 7.5%), chordae and papillary muscle (2 V, 3.8%) and one vegetation (9%) in each of the following: pulmonic valve, inferior vena cava, eustachian valve, and right atrium. The most common location for vegetations was the anterior leaflet of the tricuspid valve (19 V, 35.8 %) followed by the posterior leaflet (11 V, 20.8%). The most common vegetations morphology was raceme-like shaped (35.8%). Staphylococcus aureus (S. aureus) was the most common causative pathogen (14 pts, 50%). The incidence of PE was very high in patients with vegetation length above 1.5 cm (median 17.6±6.5 mm by TEE). Our results suggest that a routine CTPA should be advised in the presence of vegetations larger than 1.5 cm and with S. aureus infection. This behavior would identify patients at high risk of PE who will benefit from a more aggressive therapeutic strategy, leading to an improvement in the prognosis. Further prospective studies are required to better confirm our hypothesis.




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- Ananda Datta, Satya Padmaja Mantha, Suvradeep Mitra, Prasanta Raghab Mohapatra, M Srikanth Goud, Manoj Kumar Panigrahi, ROS1 positive non-small cell lung cancer with pulmonary embolism in a 22-year woman , Monaldi Archives for Chest Disease: Vol. 90 No. 3 (2020)
- Richa Tyagi, Surya Kant, Sanjeev Kumar Verma, Ram Awadh Singh Kushwaha, Santosh Kumar, Rajiv Garg, Ajay Kumar Verma, Anand Srivastava, Darshan Kumar Bajaj, Anupam Wakhlu, Anit Parihar, Akshyaya Pradhan, Riddhi Jaiswal, Spectrum of interstitial lung diseases and their association with pulmonary hypertension , Monaldi Archives for Chest Disease: Vol. 92 No. 3 (2022)
- Swetabh Purohit, Manu Madan, Rohit Kumar, Rajnish Kaushik, Pranav Ish, Mahendran AJ, Shibdas Chakrabarti, Neeraj Kumar Gupta, Nitesh Gupta, Comparison of immediate withdrawal and stepwise reduction in duration of non-invasive ventilation in chronic obstructive pulmonary disease patients presenting with acute hypercapnic respiratory failure , Monaldi Archives for Chest Disease: Early Access
- Pankti Sheth Ketan, Rohit Kumar, Mahendran AJ, Pranav Ish, Shibdas Chakrabarti, Neeraj Kumar Gupta, Nitesh Gupta, Post-extubation high-flow nasal cannula oxygen therapy versus non-invasive ventilation in chronic obstructive pulmonary disease with hypercapnic respiratory failure , Monaldi Archives for Chest Disease: Vol. 94 No. 2 (2024)
- Michele Vitacca, Marta Lazzeri, Enrico Guffanti, Pamela Frigerio, Francesco D’Abrosca, Silvia Gianola, Mauro Carone, Mara Paneroni, Piero Ceriana, Franco Pasqua, Paolo Banfi, Francesco Gigliotti, Carla Simonelli, Serena Cirio, Veronica Rossi, Chiara G. Beccaluva, Mariangela Retucci, Martina Santambrogio, Andrea Lanza, Francesca Gallo, Alessia Fumagalli, Marco Mantero, Greta Castellini, Mariaconsiglia Calabrese, Giorgio Castellana, Eleonora Volpato, Marina Ciriello, Marina Garofano, Enrico Clini, Nicolino Ambrosino, on behalf of AIPO, ARIR, SIP, AIFI and SIFIR, An Italian consensus on pulmonary rehabilitation in COVID-19 patients recovering from acute respiratory failure: results of a Delphi process , Monaldi Archives for Chest Disease: Vol. 90 No. 2 (2020)
- Emanuela Barisione, Giovanni A. Rossi, Mario Salio, Gradually worsening dyspnea and dry cough in an elderly patient , Monaldi Archives for Chest Disease: Vol. 87 No. 2 (2017)
- Costantina Prota, Rodolfo Citro, Angelo Silverio, Roberto Ascoli, Corrado Naddeo, Giovanni Vitale, Federico Piscione, Thrombus straddling a patent foramen ovale , Monaldi Archives for Chest Disease: Vol. 80 No. 3 (2013): Cardiac series
- Raffaele Griffo, Antonio Spanevello, Pier Luigi Temporelli, Pompilio Faggiano, Mauro Carone, Giovanna Magni, Nicolino Ambrosino, Luigi Tavazzi, Italian survey on prevalence and disease management of chronic heart failure and chronic obstructive pulmonary disease comorbidity in ambulatory patients. SUSPIRIUM study rationale and design , Monaldi Archives for Chest Disease: Vol. 82 No. 1 (2014): Cardiac series
- Halil Yanardag, Cuneyt Tetikkurt, Muammer Bilir, Clinical and prognostic significance of muscle biopsy in sarcoidosis , Monaldi Archives for Chest Disease: Vol. 88 No. 1 (2018)
- D.P. Tashkin, Smoked Marijuana as a Cause of Lung Injury , Monaldi Archives for Chest Disease: Vol. 63 No. 2 (2005): Pulmonary series
<< < 3 4 5 6 7 8 9 10 11 12 > >>
You may also start an advanced similarity search for this article.
