Effectiveness of early awake self proning strategy in non-intubated patients with COVID-19 hypoxemia: an open-labelled randomized clinical trial from Jodhpur, India
Accepted: December 5, 2022
Supplementary: 146
Supplementary 2_Ethics-Trial: 103
Supplementary 3-CONSORT Checklist: 135
Supplementary 4-Ministry of Health and Family Welfare handout: 95
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
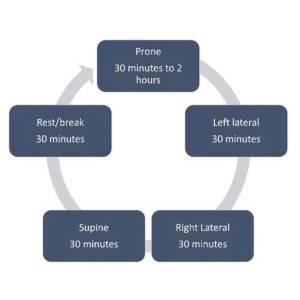
Awake self-proning is being used widely as respiratory support in COVID-19 hypoxemia, in resource-limited settings. We aimed to investigate the effectiveness of early awake self-proning in preventing mortality and the need for intubation in adults with moderate COVID-19 hypoxemia. In this randomized clinical trial with intention-to-treat analysis, we enrolled eligible adults with COVID-19 hypoxemia (SpO2 <94%), requiring supplemental oxygen via nasal prongs or facemask from a tertiary-care setting in Jodhpur, India between June 15 to December 24, 2020. Awake proning comprised of 4-hour cycles with prone position maintained 2 h per cycle. The control group did not maintain any specific position. All participants received standard care. The primary outcomes were 30-day mortality and requirement for mechanical ventilation. Of 502 participants included, mean (SD) age was 59.7 (12.7) years with 124 women (24.6%); 257 were randomized to awake-proning, 245 to control group and all 502 were included for follow-up mortality analysis. Mortality at follow-up was 16.3% in the awake-prone and 15.1% in the control group [OR:1.10 (0.68-1.78), p=0.703). The requirement of mechanical ventilation was 10% in both groups (p=0.974). Survival time (in days) was not significantly different between the groups [Log-rank test, HR: 1.08 (95% CI, 0.70-1.68), p=0.726]. Likewise, time to intubation was comparable (Log-rank test, HR: 0.93 (95% CI, 0.56-1.70), p=0.974). Hence, awake self-proning did not improve survival or requirement of mechanical-ventilation in non-intubated patients with mild to moderate COVID-19 hypoxemia. Trial Registration: Clinical trial registry of India, ID: CTRI/2020/06/025804.
The trial is accessible from WHO's International Clinical Trials Registry Platform (ICTRP) at https://trialsearch.who.int
***************************************************************
*Appendix Authors list
Deepak Kumar1, Gopal Krishna Bohra1, Nishant Kumar Chauhan2, Nikhil Kothari3, Vijaya Lakshmi Nag4 Sanjeev Misra5
1Department of Internal Medicine; 2Department of Pulmonary Medicine; 3Department of Anaesthesiology and Critical Care; 4Department of Microbiology; 5Department of Surgical Oncology, All India Institute of Medical Sciences, Jodhpur, India




Ethics Approval
the study was approved by Institute Ethics Committee (AIIMS/IEC/2020-21/2040)., Trial was registered at Clinical trial registry of India, CTRI/2020/06/025804 and is accessible from WHO's International Clinical Trials Registry Platform (ICTRP) at https://trialsearch.who.inHow to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
Similar Articles
- Muhammad Ijaz, Muhammad Jaffar Khan, Jawad Khan, . Usama, Association of clinical characteristics of patients presenting with influenza like illness or severe acute respiratory illness with development of acute respiratory distress syndrome , Monaldi Archives for Chest Disease: Vol. 87 No. 1 (2017)
- Massimiliano Polastri, Lara Pisani, Andrea Dell'Amore, Stefano Nava, Revolving door respiratory patients: A rehabilitative perspective , Monaldi Archives for Chest Disease: Vol. 87 No. 3 (2017)
- Michele Vitacca, Luca Barbano, Daniele Colombo, Olivia Leoni, Enrico Guffanti, Prevalence and variability of use of home mechanical ventilators, positive airway pressure and oxygen devices in the Lombardy region, Italy , Monaldi Archives for Chest Disease: Vol. 88 No. 1 (2018)
- Gabriele Valli, Francesca De Marco, Maria Teresa Spina, Valentina Valeriano, Antonello Rosa, Valentina Minerva, Enrico Mirante, Maria Pia Ruggieri, Francesco Rocco Pugliese, A pilot study on the application of the current European guidelines for the management of acute coronary syndrome without elevation of ST segment (NSTEMI) in the Emergency Department setting in the Italian region Lazio , Monaldi Archives for Chest Disease: Vol. 82 No. 4 (2014): Cardiac series
- S. Bertini, M. Picariello, M. Gorini, T. Renda, A. Augustynen, G. Villella, G. Misuri, N.M. Maluccio, R. Ginanni, D. Tozzi, A. Corrado, Telemonitoring in chronic ventilatory failure: a new model of survellaince, a pilot study , Monaldi Archives for Chest Disease: Vol. 77 No. 2 (2012): Pulmonary series
- F. Novelli, F. Costa, M. Latorre, L. Malagrinò, A. Celi, B. Vagaggini, P. Paggiaro, Tiotropium: a new therapeutic option in asthma , Monaldi Archives for Chest Disease: Vol. 79 No. 3-4 (2013): Pulmonary series
- Samuele Baldasseroni, Francesco Orso, Alessandra Pratesi, Alice Foschini, Andrea Giosafat Marella, Nadia Bartoli, Ilaria Bracali, Alessando Antenore, Francesca Tarantini, Costanza Burgisser, Niccolò Marchionni, The complexity of risk stratification in older patient candidate to non-cardiac surgery , Monaldi Archives for Chest Disease: Vol. 78 No. 3 (2012): Cardiac series
- Francesco Barillà , Concetta Torromeo, Riccardo Iorio, Luigina Porco, Vincenzo Paravati, Carlo Gaudio, Antiplatelet therapy in elderly patients with acute coronary syndrome: Between scientific evidence and future perspectives , Monaldi Archives for Chest Disease: Vol. 88 No. 2 (2018)
- A. Chroneou, N. Zias, A.V. Gonzalez, J.F. Beamis Jr, Tracheobronchopathia Osteochondroplastica. An underrecognized entity? , Monaldi Archives for Chest Disease: Vol. 69 No. 2 (2008): Pulmonary series
- M. Vitacca, L. Bianchi, L. Barbano, N. Ambrosino, Lung and respiratory muscle function at discharge from a respiratory intensive care unit , Monaldi Archives for Chest Disease: Vol. 63 No. 3 (2005): Pulmonary series
You may also start an advanced similarity search for this article.
